
BU Identifies Biomarker That Could Allow The Living To Be Tested For CTE

 Chris Nowinski and Dr. Ann McKee at a House Judiciary Committee hearing in 2009 (photo via Charles Dharapak/ [object Object] )
Chris Nowinski and Dr. Ann McKee at a House Judiciary Committee hearing in 2009 (photo via Charles Dharapak/ [object Object] ) Boston University’s CTE Center released a study yesterday detailing research on a protein found in spinal fluid that, they say, “may be a novel target for future CTE biomarker studies” that could eventually be part of a panel of tests to identify chronic traumatic encephalopathy—the pathology at the center of football’s brain-injury crisis—in the living. (Currently, CTE can only be diagnosed post-mortem by an examination of built-up tau proteins in brain tissue.)
Additionally, the protein may help further distinguish CTE from Alzheimer’s disease, which is also identifiable by a build-up of tau proteins. CTE presents similarly to Alzheimer’s, dementia, or simply the cognitive deterioration of old age, so any and all research that uniquely identifies CTE works to solidify its still-controversial recognition as a distinct pathology.
The protein BU researchers are saying may be an indicator of CTE is called CCL11. Last year, BU researchers identified a correlation between persistent brain inflammation and the development of tau proteins and worsening of CTE in a subject. CCL11, comparatively, has been shown to “play a role in neuroinflammation and neurodegeneration. CCL11 levels increase in the plasma and cerebrospinal fluid (CSF) of mice and humans as part of normal aging. In mice, these increases are associated with declining neurogenesis and impaired cognition and memory,” per the BU study.
The researchers studied the spinal fluid of 23 men who had played football, ranging from ages 25 to 87, 50 people who had been neuropathically diagnosed with Alzheimer’s disease, and 18 non-athlete control subjects. What they found:
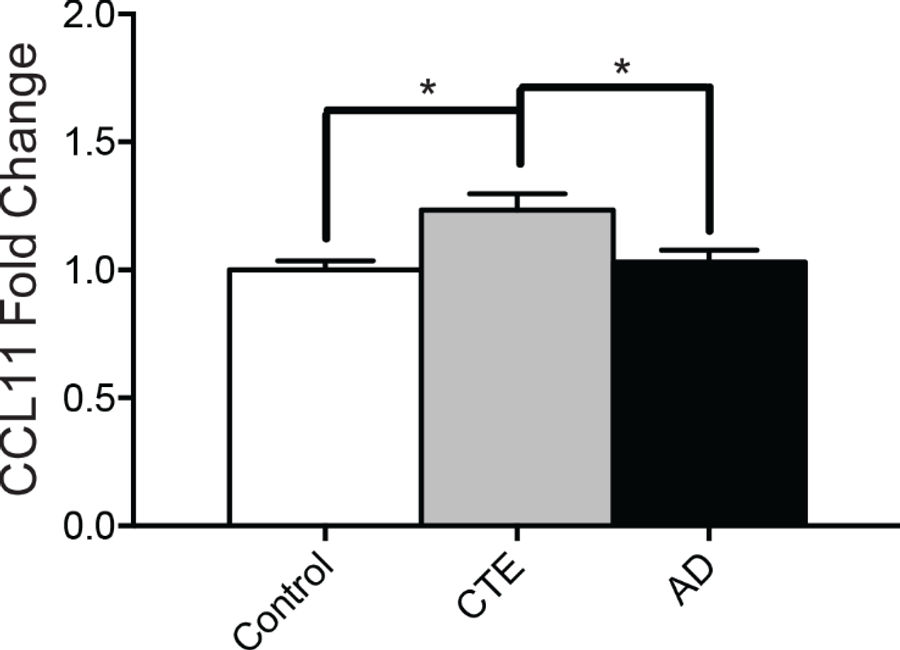
... levels of CCL11 were significantly increased in subjects with CTE compared to controls or to subjects with AD.
Furthermore, when pooling the control, AD, and CTE subjects together, a binary logistic regression was able to significantly discriminate a positive neuropathologic diagnosis of CTE when using CCL11 fold changes.
Simply put, CTE subjects had more CCL11, and researchers were able to distinguish CTE subjects from Alzheimer’s and control subjects based on their CCL11 levels. In this small sample, researchers were able to diagnose CTE based on the CCL11 in their spinal fluid.
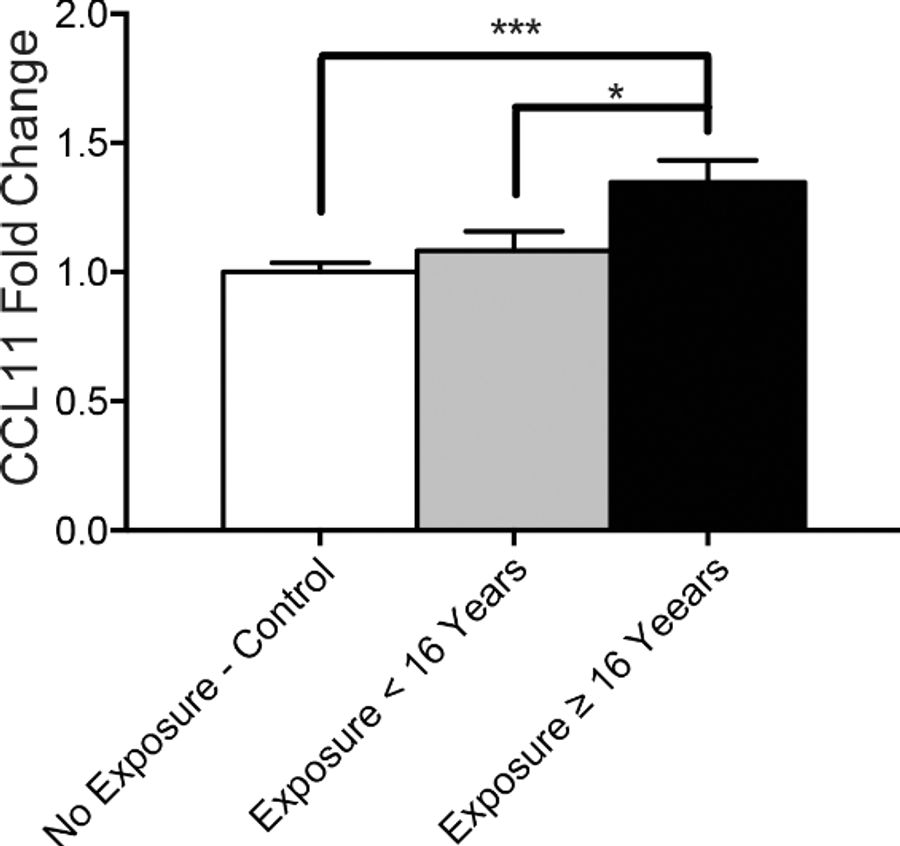
Additionally, the researchers found a correlation between total years of football played and the amount of CCL11 in a person’s cerebrospinal fluid. Subjects who played football for 16 or more years had “a significant increase in CCL11 levels” compared to every other subject in the study.
Here are two graphs included in the study that show very simply the variation the researchers found across the samples:
The takeaway here is that this is a small but real breakthrough in progress toward developing a way to diagnose CTE in the living. (BU’s research into CCL11 protein, it should be noted, is work distinct from that done in a UCLA study—which has been the subject of massive controversy—which aims to identify the levels of tau proteins in the living.) Once researchers are able to definitively make a diagnosis, they can begin to research treatment options for those suffering from the disease. This study—which, again, examined only 23 former football players—is very preliminary, and it will be years, if not decades, before we use this research to help those experiencing the symptoms of CTE while alive.
Still, advances in research into identifying CTE in the living are genuinely the biggest threat that exists to the future of American football as we know it. What could end the NFL as we know it isn’t television ratings, and it isn’t protests during the national anthem; it’s definitive CTE diagnoses in the living.
Fans, families, and players have been justifiably alarmed by diagnoses of CTE post-mortem, especially in big-name former players such as Frank Gifford or Junior Seau. Last week’s news that Aaron Hernandez had a severe case of CTE at age 27 just makes the alarm sound a bit louder—even if the idea that the disease drove him to commit his crimes is neat and potentially dangerous.
But the potential to identify CTE in the living would mean, essentially, that the jig is up for football, if the strong correlation between football (or repetitive, sub-concussive brain trauma) and CTE persists as research develops to include a wider array of subjects. When players (and parents) are able to see, in real time, the potential results of those hits, it will present a scandal that football at all levels stands little chance of navigating.
It will make the ever-growing crisis one that can’t be ignored. It will discourage more families from putting their kids into football to begin with, and we will see more and more players walk away from the game before their prime. And despite the NFL’s assurances that football is safer than ever—part of their attempt to brush away CTE as a problem mostly for older players who played the game before better helmets and more penalty flags—there is simply no way to have American football as we know it without hits and g-force to the head on basically every play.
The curse of CTE research is that its association with the most popular sport in America means that every single development gets a spray of headlines, thrusting preliminary research into the public eye. Some day, there will be a test that identifies CTE in the living, and the reckoning will come. BU’s latest study may or may not be a foundational element of that test, but it’s an advance. As Dr. Cherry told me, “what we’re trying to convey is that this is the first step, but it is a very, very promising first step.”










- Best NBA Betting Picks and Predictions for Monday April 6th
- National Championship Bet Pick: Why Michigan Has the Edge Over UConn
- UFC Vegas 115 Betting Picks: Moicano vs. Duncan Headlines April 4th Card
- NBA Betting Picks April 4th: Three Best Bets for Saturday's Slate
- Michigan vs. Arizona Bets: Wolverines Hold Edge in Final Four Showdown
- Best NBA Betting Picks Today: Friday April 3rd Expert Predictions
- MLB Pitcher Props Today: Best Baseball Bets for April 3rd
